How Common Are Prominent Ears, and Why Does It Matter?
Prominent ears, sometimes called protruding or "sticky-out" ears, are one of the most common congenital ear deformities. Research published in the National Library of Medicine estimates that approximately 5% of the Caucasian population has ears that protrude more than 2 cm from the side of the head, a threshold generally considered outside the typical range (PubMed, 2020).
Despite being a purely cosmetic variation with no effect on hearing or physical health, prominent ears carry a disproportionate psychological burden. Decades of research in developmental psychology, plastic surgery outcomes, and pediatric mental health have documented measurable effects on self-esteem, social functioning, and quality of life. For many people, the impact begins in early childhood and persists well into adulthood.
This article examines the research behind those psychological effects, explores what parents can do to support children who are teased, and outlines evidence-based coping strategies for people of all ages.
What the Research Says About Psychological Impact
Facial Perception and First Impressions
The ears play a more significant role in facial perception than most people assume. A study published in JAMA Facial Plastic Surgery found that faces with protruding ears were perceived differently across multiple social dimensions. Participants rated individuals with prominent ears as less attractive, less successful, and less intelligent compared to the same faces digitally altered to show non-protruding ears. These judgments were made within seconds and remained consistent across demographic groups.
This finding aligns with broader research on the "halo effect," a cognitive bias where physical appearance influences assumptions about a person's character and competence. When ears fall outside socially expected proportions, they can trigger unconscious negative appraisals.
Self-Esteem and Body Image
Multiple studies have linked prominent ears to lower self-esteem scores, particularly during childhood and adolescence. A 2018 systematic review in the Journal of Plastic, Reconstructive & Aesthetic Surgery found that children with prominent ears scored significantly lower on validated self-esteem inventories than age-matched peers. The effect was most pronounced between ages 6 and 14, the period when peer comparison intensifies and physical appearance becomes closely tied to social acceptance.
Among adults, the relationship is more variable. Some individuals report that self-consciousness diminishes with age, while others describe a persistent awareness that shapes behavior: choosing hairstyles to cover the ears, avoiding social situations, or feeling anxious in photographs.
Bullying and Social Exclusion
Perhaps the most concerning research relates to bullying. A study published in PMC found that otoplasty (surgical ear correction) reduced bullying incidents by approximately 70% in school-age children (PMC, 2024). While this statistic speaks to the effectiveness of surgical intervention, it also reveals the severity of the problem: if correcting the ears reduces bullying by that margin, the ears themselves were a primary target.
A survey conducted in the UK by the charity Changing Faces found that approximately 60% of children with a visible facial difference (including prominent ears) reported being bullied at school. Children with prominent ears specifically reported names like "Dumbo" or "satellite ears," terms that may sound trivial to adults but carry real weight in the social hierarchies of childhood.
Children and Bullying: School-Age Impacts
When Teasing Becomes Harmful
There is a meaningful distinction between occasional teasing and sustained bullying, and the threshold is lower than many adults recognize. A single comment about a child's ears may be forgotten within a day. Repeated comments, especially from multiple peers, can reshape a child's self-concept over time.
Research in developmental psychology identifies several warning signs that teasing about physical appearance has crossed into harmful territory:
- The child begins avoiding activities they previously enjoyed (especially those requiring helmets, headbands, or being photographed)
- They express a desire to change their appearance or ask to cover their ears with hats or hairstyles
- They become withdrawn, irritable, or reluctant to attend school
- They report feeling "ugly," "weird," or "different" from peers
- Sleep disturbances, appetite changes, or physical complaints (headaches, stomachaches) emerge without medical cause
What Parents Can Do
Parents occupy a critical position. They are often the first to notice a shift in their child's mood and the most trusted source of emotional support during formative years. Research-supported strategies include:
- Validate their experience. Avoid minimizing ("It's not a big deal") or dismissing ("Just ignore them"). Instead, acknowledge the emotional reality: "That sounds really frustrating. I understand why it hurt your feelings."
- Teach response skills. Role-play scenarios where the child practices calm, confident responses to teasing. Even simple phrases ("Yeah, my ears are bigger. So what?") can reduce a bully's leverage by removing the expected emotional reaction.
- Engage the school. Many schools have anti-bullying protocols. If teasing is persistent, parents should document incidents and request a meeting with the child's teacher or school counselor.
- Monitor but don't overcorrect. Drawing excessive attention to the ears at home can amplify a child's self-consciousness. Focus on building general resilience and self-worth rather than centering conversations on the ears specifically.
- Consider professional support early. If a child's self-esteem, school performance, or social life is noticeably affected, a few sessions with a child psychologist can provide tools that last a lifetime.
Adult Self-Consciousness: How Childhood Insecurity Carries Forward
A 2019 study in Aesthetic Surgery Journal surveyed adults seeking otoplasty and found that over 75% traced their dissatisfaction to experiences in childhood or adolescence. Many described decades of avoidance behaviors: never wearing their hair up, sitting in specific positions to hide their ears, or declining to be photographed from certain angles.
Psychologists describe this as a form of body-focused repetitive behavior (when it involves checking or adjusting) or appearance-related avoidance (when it involves hiding). In more severe cases, persistent preoccupation with ear appearance may meet the clinical criteria for body dysmorphic disorder (BDD), a condition where perceived flaws in appearance cause significant distress and functional impairment.
It is important to note that BDD is not simply "being self-conscious." It is a diagnosable condition with effective treatments. Not everyone who dislikes their ears has BDD, but for those who spend hours a day thinking about their ears, avoid social situations, or experience severe anxiety related to their appearance, a professional evaluation is warranted.
The Social and Professional Impact
Adults with prominent ears report effects that extend beyond personal insecurity into professional and social domains:
| Domain | Reported Impact |
|---|---|
| Workplace | Reluctance to present in meetings, avoidance of video calls, choosing roles with less visibility |
| Dating and relationships | Anxiety about a partner seeing ears without concealment, avoidance of physical intimacy in bright lighting |
| Social activities | Declining invitations to swimming, sports, or outdoor events where hair may shift or hats are impractical |
| Photography | Avoiding group photos, insisting on certain angles, feeling anxious about social media tagging |
These patterns often operate beneath conscious awareness. Recognizing them as responses to a specific insecurity, rather than "just how I am," is often the first step toward change.
Evidence-Based Coping Strategies
Psychological research has identified several approaches that help people reduce distress related to physical appearance concerns, including prominent ears. These are not quick fixes, but practiced consistently, they produce measurable improvements in self-esteem and quality of life.
Cognitive Behavioral Techniques (CBT)
CBT is the most studied psychological intervention for appearance-related distress. It works by identifying and restructuring distorted thought patterns. Common cognitive distortions related to prominent ears include:
- Mind reading: "Everyone is staring at my ears."
- Catastrophizing: "If someone sees my ears, they'll think I look ridiculous."
- All-or-nothing thinking: "I can never look good with these ears."
- Filtering: Noticing one person's glance while ignoring dozens of neutral or positive interactions.
A CBT approach involves recording these thoughts, evaluating the evidence for and against them, and generating more balanced alternatives. For example, "Everyone is staring at my ears" might be reframed as: "I notice my ears more than other people do. Most people are focused on their own concerns."
Self-Compassion Practice
Research by Dr. Kristin Neff and colleagues has shown that self-compassion, treating yourself with the same kindness you would offer a friend, is strongly associated with lower body dissatisfaction and higher psychological resilience. Self-compassion involves three components:
- Self-kindness over self-judgment. Instead of "I hate how my ears look," try "I'm struggling with how I feel about my ears, and that's a difficult experience."
- Common humanity over isolation. Approximately 5% of the population shares this trait. Millions of people navigate the same feelings.
- Mindfulness over over-identification. Notice the thought ("I'm thinking about my ears again") without fusing with it or acting on it.
Behavioral Experiments
One of the most effective (and most uncomfortable) techniques involves deliberately testing feared outcomes. For someone who always covers their ears with their hair, a behavioral experiment might involve wearing their hair up in a low-stakes environment and observing what actually happens. In nearly all cases, the feared reaction (people staring, laughing, commenting) does not occur, which weakens the anxious belief over time.
Gradual Exposure
Related to behavioral experiments, gradual exposure involves slowly increasing comfort with situations that trigger self-consciousness. A structured exposure hierarchy might look like this:
- Looking at photos of yourself with ears visible (alone, privately)
- Wearing hair up at home around family
- Wearing hair up on a short errand (grocery store, gas station)
- Wearing hair up at work or school
- Allowing photos to be taken without controlling the angle
Each step is repeated until the anxiety decreases meaningfully before moving to the next. This process, called habituation, is one of the most reliable mechanisms of anxiety reduction in clinical psychology.
Non-Surgical Options: A Balanced Overview
For people who want to reduce ear protrusion without surgery, several options exist. Each has trade-offs in terms of effectiveness, cost, and convenience.
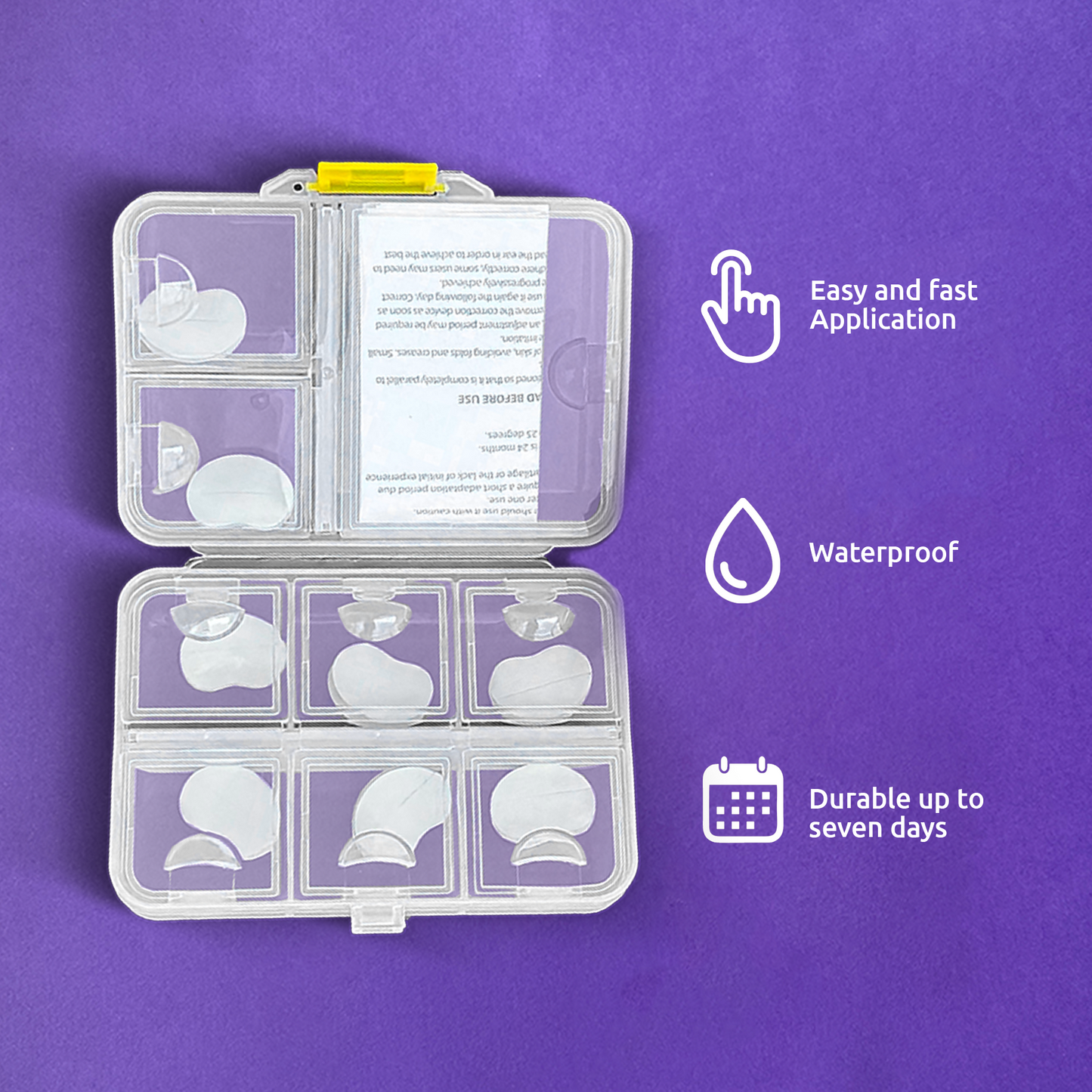
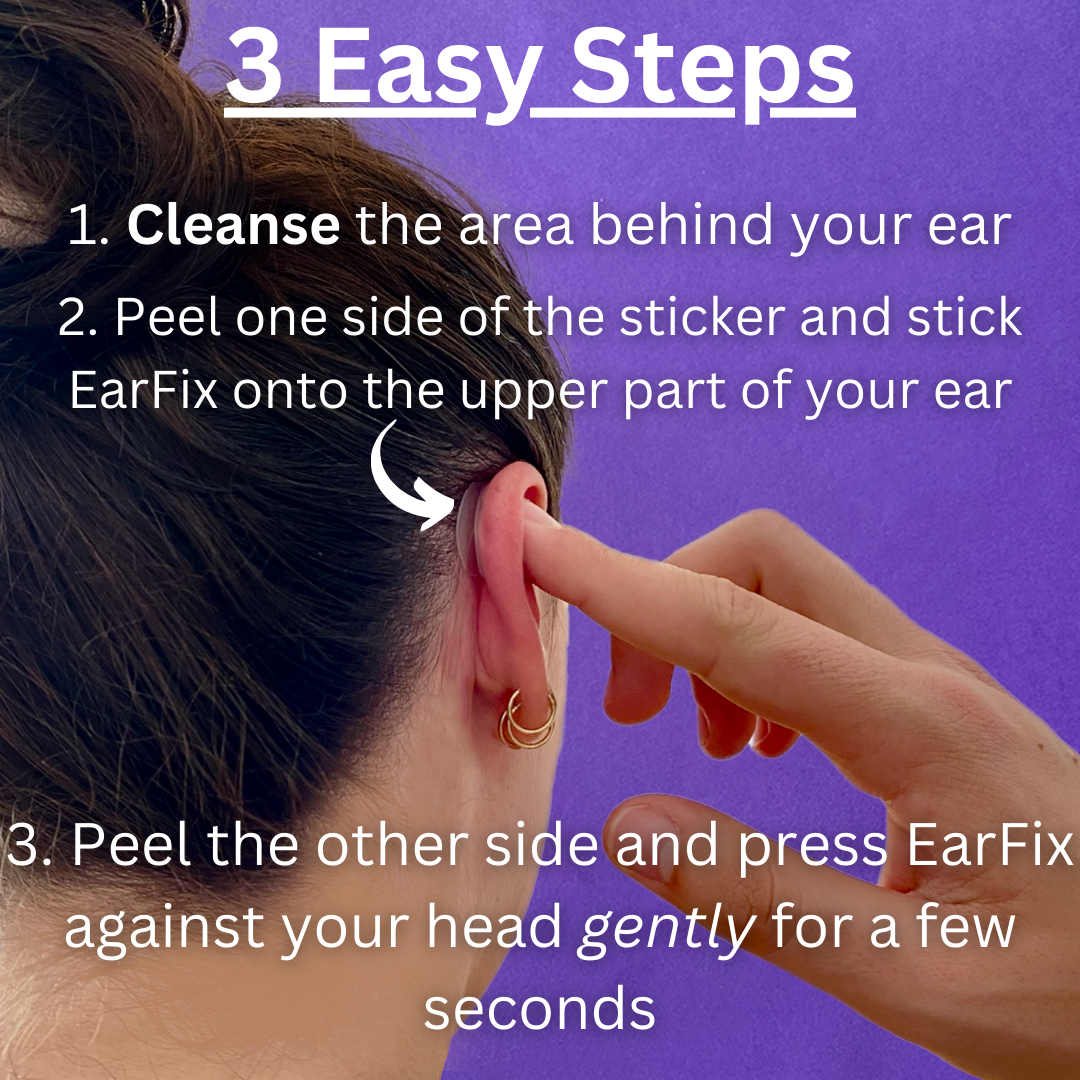
Adhesive Ear Correctors
Adhesive correctors are small, transparent stickers or tape strips that hold the ear closer to the head. They are the most popular non-surgical option because they provide an immediate visual change, are invisible to others when applied correctly, and can be removed at any time. Products like EarFix ear correctors are designed to be discreet and comfortable for daily wear. Adhesive correctors work well for social events, photos, or everyday use, though they are a cosmetic solution rather than a permanent structural change.
Hairstyling
Many people choose hairstyles that partially or fully cover the ears. While effective at concealment, this approach can become limiting over time, especially in hot weather, during physical activity, or in professional settings where certain hairstyles are impractical. Relying exclusively on hairstyling may also reinforce avoidance patterns that psychologists recommend addressing directly.
Ear Molding for Infants
For newborns with prominent ears, ear molding (using splints or molds to reshape the soft cartilage) has a high success rate when started within the first few weeks of life. A study in Plastic and Reconstructive Surgery reported over 90% effectiveness when treatment began before 3 months of age. This option is time-sensitive and requires guidance from a pediatrician or specialist.
Otoplasty
Surgical correction (otoplasty) remains the only permanent solution for repositioning the ears. It is typically performed on children aged 5 and older or on adults. Recovery time ranges from 1 to 2 weeks, and patient satisfaction rates are generally high, with studies reporting satisfaction above 90% at one-year follow-up. Otoplasty is discussed further in the professional help section below.
When to Seek Professional Help
Therapy and Counseling
If self-consciousness about your ears is affecting your daily life, relationships, or mental health, speaking with a therapist is a productive step. Look for a psychologist or counselor who specializes in:
- Body image concerns or body dysmorphic disorder
- Cognitive behavioral therapy (CBT), which has the strongest evidence base for appearance-related distress
- Acceptance and commitment therapy (ACT), which focuses on living well alongside difficult thoughts rather than eliminating them
The goal of therapy is not necessarily learning to "love your ears." It is reducing the degree to which appearance concerns control your decisions and limit your activities.
When Surgery Might Be Appropriate
Otoplasty is a reasonable consideration when:
- The psychological distress is significant and persistent (lasting years, not weeks)
- Non-surgical approaches have been explored and found insufficient
- The motivation is internal (the person wants it for themselves, not because someone else suggested it)
- Expectations are realistic (surgery changes ear position, not overall life satisfaction)
For children, most surgeons recommend waiting until age 5 or 6, when the ear cartilage is firm enough for reliable correction. Parental motivation alone is not sufficient; the child should express their own desire for the procedure. A consultation with a board-certified plastic surgeon or otolaryngologist can clarify what results are realistic. For a broader look at options, see our guide on how to fix ears that stick out.
Frequently Asked Questions
At what age are children most affected by teasing about their ears?
Research consistently identifies ages 6 through 14 as the highest-risk period. This is when children become acutely aware of physical differences, peer acceptance becomes a primary social motivator, and teasing is most common. However, the psychological effects often extend well beyond these years, with many adults reporting that childhood teasing shaped their self-image long-term.
Can prominent ears cause clinical anxiety or depression?
Prominent ears themselves do not cause anxiety or depression, but the social experiences associated with them (bullying, exclusion, negative self-perception) can contribute to both. In severe cases, persistent preoccupation with ear appearance may meet the criteria for body dysmorphic disorder. If appearance concerns are interfering with your daily functioning, a mental health professional can provide an accurate assessment.
Do non-surgical options like adhesive correctors help with self-confidence?
Many people report improved confidence when using adhesive correctors like EarFix, particularly in situations where they feel most self-conscious (photos, social events, video calls). They can serve as a practical tool while someone works on deeper psychological strategies, or as a standalone solution for occasional use. The key is ensuring they supplement confidence-building rather than replace it entirely.
Is otoplasty safe for children?
Otoplasty is considered a safe procedure with a low complication rate when performed by a qualified surgeon. The American Society of Plastic Surgeons notes that it is one of the most common pediatric cosmetic procedures. Potential risks include infection, asymmetry, and dissatisfaction with results, though these occur in a small minority of cases. Most children return to school within 1 to 2 weeks.
How can I tell if my concern about my ears is normal or something I should get help for?
A useful benchmark is functional impact. If you occasionally wish your ears were different but it does not affect your behavior, that falls within the normal range of appearance awareness. If you spend significant time each day thinking about your ears, avoid activities or social situations because of them, or experience distress that feels disproportionate to the situation, professional support would be beneficial. There is no threshold you need to reach before "earning" the right to talk to a therapist.
Will my child grow out of being bothered by their ears?
Some children naturally become less concerned as they age, develop stronger social skills, and build confidence from other sources (academics, sports, friendships). Others carry the self-consciousness into adulthood. There is no reliable way to predict which path a particular child will follow. The most protective approach is to take their concerns seriously, provide emotional support, and seek professional help if their distress is escalating or persistent.