If you have been studying your newborn's ears and wondering whether they look a little more prominent than expected, take a breath. You are far from alone. Prominent ears are one of the most common cosmetic variations in newborns, and in almost every case, they have zero impact on hearing or health. But that does not mean your concerns are trivial. This guide covers everything parents need to know: why baby ears stick out, the science behind the critical cartilage window, your correction options, realistic timelines, costs, and when to talk to your pediatrician.
Why Do Some Baby Ears Stick Out?
Prominent ears in babies typically come down to three factors working together: genetics, womb positioning, and the natural softness of infant ear cartilage.
Genetics
Ear shape is heritable, just like eye color or nose shape. If prominent ears run in your family (yours, your partner's, or either set of grandparents), there is a good chance your baby inherited the trait. Research published in the Journal of Craniofacial Surgery estimates that approximately 5% of the Caucasian population has clinically prominent ears, though rates vary across ethnicities. A study of Zimbabwean primary school children found a prevalence of about 6.89%.
Womb Positioning
During the final weeks of pregnancy, space in the uterus gets tight. A baby's soft ears can be folded or pressed against the uterine wall for weeks at a time, temporarily shaping them into a more prominent position at birth.
Cartilage Structure
Prominent ears usually involve one of two anatomical features:
- Underdeveloped antihelical fold: The antihelix is the inner ridge that gives the ear its curved shape. When this fold is shallow or absent, the outer ear projects outward instead of curving back toward the head.
- Excess conchal cartilage: The concha is the bowl-shaped area near the ear canal. Extra cartilage here pushes the entire ear away from the skull.
Neither variation affects hearing. They are purely cosmetic differences in ear anatomy.
Is It Normal for Newborn Ears to Stick Out?
Yes. Newborn ear variations are remarkably common. A 2015 study published in Plastic and Reconstructive Surgery examined thousands of newborns and found that roughly 20 to 35% of all newborns are born with some form of ear shape irregularity, including prominent ears, folded helixes, and asymmetry. Many of these are mild and temporary, but not all resolve on their own.
A separate analysis found that only about 30% of untreated prominent ears self-correct by age one. For the remaining 70%, the ear shape present in the first months of life tends to become permanent as the cartilage hardens. This is the core reason pediatric specialists increasingly recommend early, non-surgical intervention rather than a "wait and see" approach.
It is also worth noting that prominent ears can sometimes develop or become more noticeable in the first three months after birth. Repeated pressure from sleeping positions or the ear bending during breastfeeding can gradually push a soft ear outward. This is another reason why monitoring ear shape during these early months, rather than assuming things will sort themselves out, is a practical step for attentive parents.
The Cartilage Window: Why the First 6 Months Matter
Newborn ear cartilage is unlike anything else in the body. Maternal estrogen, still circulating in your baby's bloodstream after birth, keeps the cartilage extraordinarily soft and pliable. Think of it like warm clay: easy to shape with gentle pressure, but once it cools and hardens, the form is set.
This biological reality creates what specialists call the "golden window" for non-surgical ear correction. Here is how the window narrows over time:
| Baby's Age | Cartilage Flexibility | Non-Surgical Success Rate |
|---|---|---|
| Birth to 3 weeks | Extremely soft (peak estrogen levels) | 90 to 96% (per multiple meta-analyses) |
| 3 to 6 weeks | Very soft (estrogen declining) | 85 to 90% |
| 6 weeks to 3 months | Moderately soft | Variable, treatment takes longer |
| 3 to 6 months | Firming | Still possible, requires more time |
| After 6 months | Substantially firmer | Significantly reduced effectiveness |
A 2022 systematic review and meta-analysis covering over 1,300 infants confirmed an overall effectiveness rate of 89.1% for non-surgical ear molding in congenital ear deformities, with success rates climbing above 90% when treatment started in the first three weeks. A large US study of 488 infants found 90% achieved good to excellent results with an average treatment duration of just 5.7 weeks, particularly when started in the first 10 days of life.
The takeaway is simple: the earlier you start, the faster and more effective the correction.
Non-Surgical Correction Options for Baby Ears
Parents have three broad paths when they notice their baby's ears stick out: watchful waiting, non-surgical molding, or surgery later in childhood. Here is how they compare.
Watchful Waiting
Cost: free. Risk: the ears may not self-correct (roughly 70% of the time), and you lose the window when non-surgical options work best. Some parents are comfortable with this approach, particularly for very mild cases.
Non-Surgical Ear Molding
This category includes medical-grade adhesive correctors and splint-based systems. They work by holding the ear in a more natural position while the soft cartilage gradually firms into its new shape. The process is entirely pain-free and non-invasive.
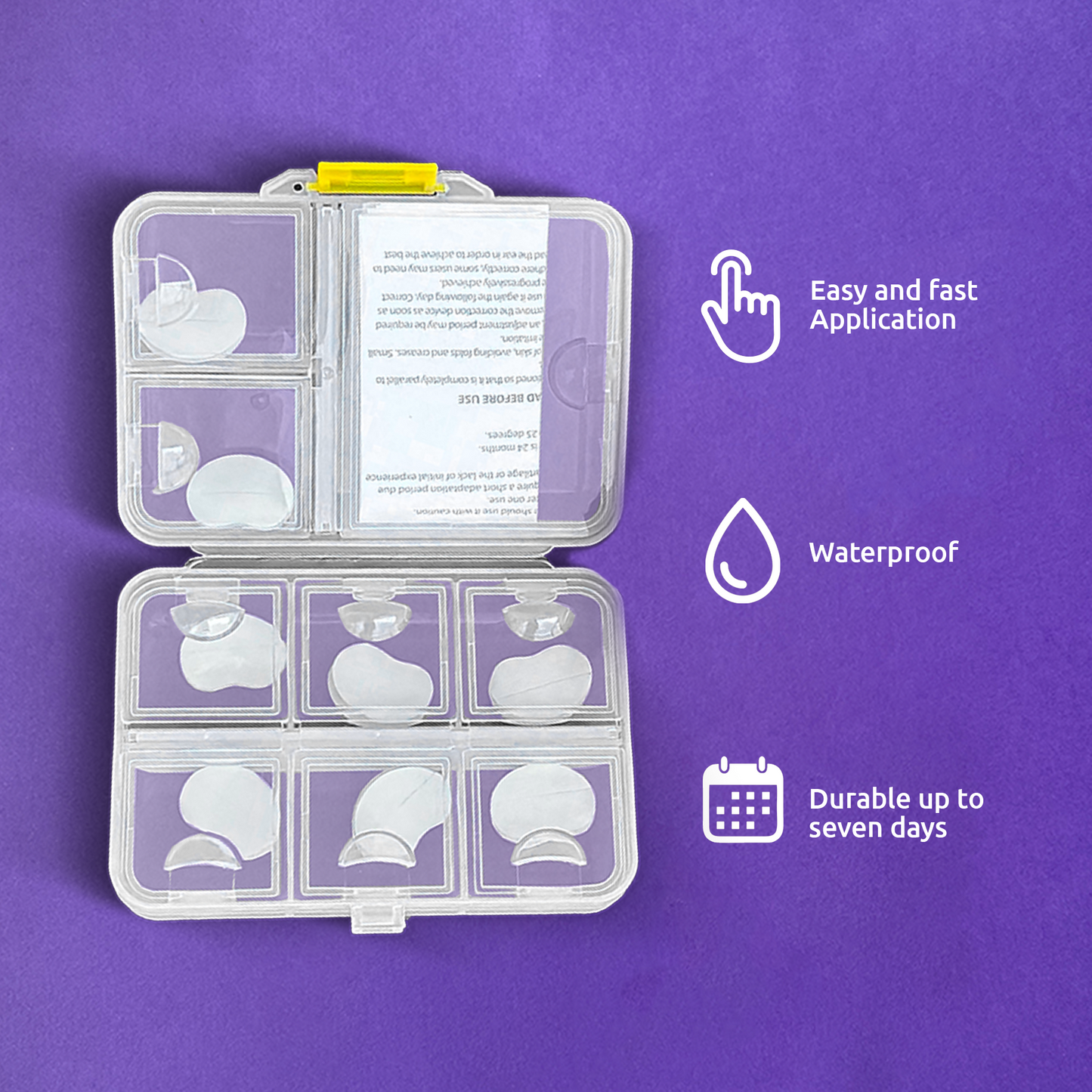
EarFix Baby is designed specifically for babies aged 3 months to 3 years. It uses transparent, medical-grade silicone correctors with a hypoallergenic, dermatologist-tested adhesive. One side attaches to the back of the ear, and the other adheres to the skin behind it, gently guiding the ear closer to the head. The correctors are waterproof, nearly invisible, and comfortable enough for 24/7 wear through naps, baths, and playtime.
Otoplasty (Surgical Correction)
Otoplasty is a formal surgical procedure typically reserved for children aged 5 and older, once the ears are nearly fully grown. It involves incisions behind the ear, cartilage reshaping, general anesthesia, and a recovery period of one to two weeks. The cost ranges from $3,000 to $8,000 or more, and it is usually considered cosmetic (not covered by insurance).
| Feature | Non-Surgical Molding | Otoplasty Surgery |
|---|---|---|
| Best age | Newborn to 6 months (ideal), up to 3 years | Age 5 and older |
| Pain level | None | Post-operative pain and swelling |
| Anesthesia | None | General or local |
| Recovery time | None | 1 to 2 weeks, activity restrictions |
| Cost | Under $50 for a full kit | $3,000 to $8,000+ |
| Risks | Occasional mild skin redness | Infection, scarring, anesthesia risks |
How Long Should Baby Ear Molding Patches Stay On?
This is one of the most common questions parents ask, and the answer depends on your baby's age at the start of treatment.
If you begin within the first few weeks of life, the entire course typically lasts 4 to 6 weeks. A clinical study tracking neonatal ear molding found patches stayed on for an average of 32 days, with a 92.6% rate of good to excellent outcomes. If you start later (2 to 6 months), expect the process to take longer, often 2 to 3 months of consistent use.
Each individual corrector patch typically lasts 3 to 7 days before it needs replacing. The adhesive gradually loosens with daily activity, and applying a fresh corrector ensures consistent gentle pressure on the cartilage.
Tips for Maximizing Wear Time
- Clean and dry skin is essential. Wash the area behind the ear with mild soap and water, then pat completely dry before applying. Skip lotions, oils, and creams on the application area.
- Avoid touching the adhesive. Handle the corrector by its edges to keep oils from your fingertips off the sticky surface.
- Apply after bath time. Your baby's skin is clean and they tend to be calm and relaxed, making placement easier.
- Press firmly for 30 to 60 seconds. Body heat helps activate the adhesive and create a secure bond.
Cost and Timing: What to Expect
A complete EarFix Baby kit costs a fraction of what you would spend on a few months of premium diapers. For newborns starting in the golden window, one kit often provides enough correctors for the full treatment course. Babies starting later may need a second kit for extended wear.
Compare that to surgical otoplasty, which averages $3,000 to $8,000 out of pocket, requires waiting until your child is at least 5, and involves anesthesia and recovery. The financial and emotional gap between these two paths is significant.
For families concerned about the investment, consider what the Newborn Butterfly Project at Weill Cornell Medicine found: their non-surgical ear molding program achieved a 96% success rate in treated infants, with parents reporting high satisfaction both in results and in the simplicity of the process.
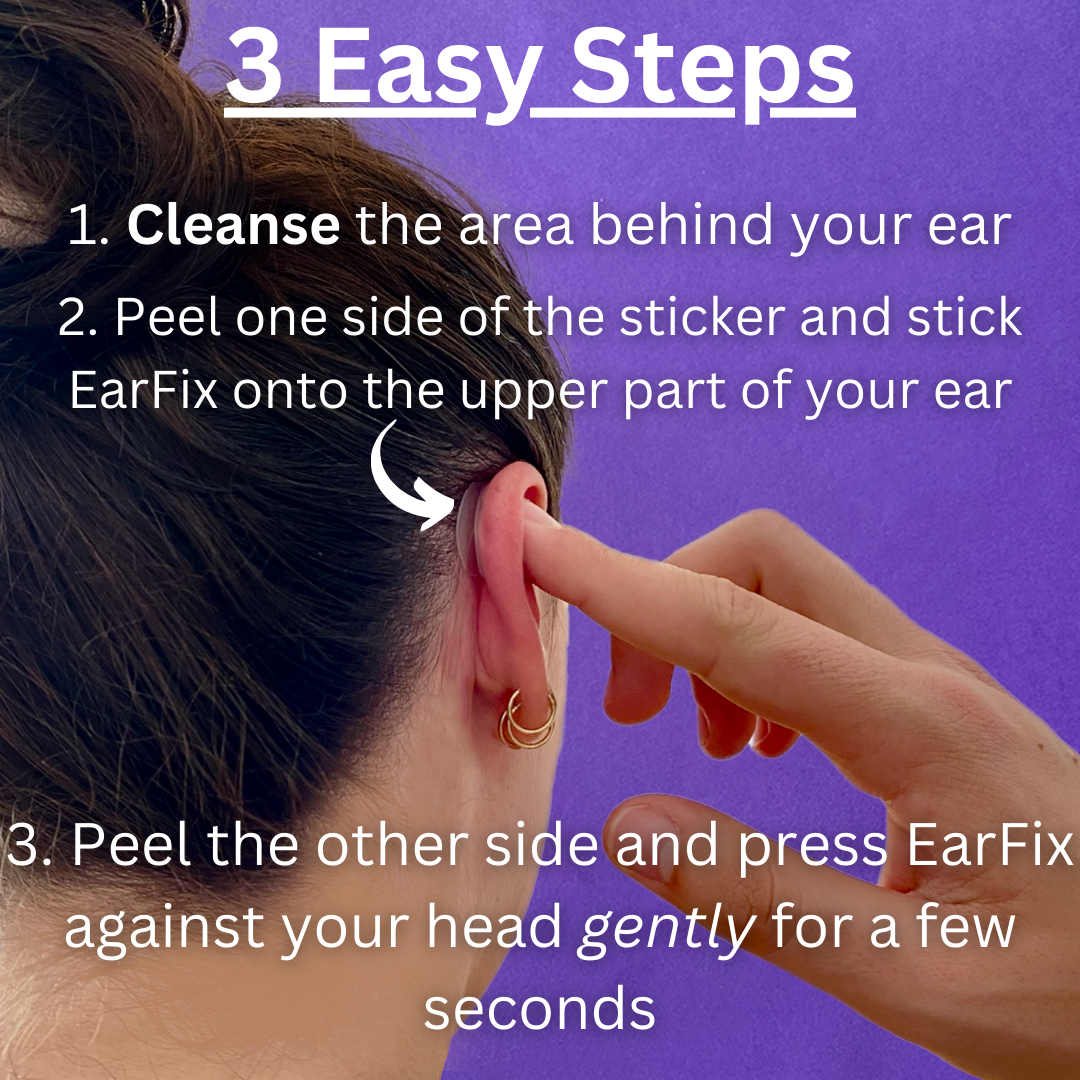
How to Apply Baby Ear Correction Stickers: Step by Step

- Clean the area. Gently wash the skin behind your baby's ear and the adjacent scalp with mild soap and water. Pat completely dry.
- Peel one side. Remove the protective backing from one side of the corrector. Avoid touching the adhesive.
- Attach to the ear. Place the exposed adhesive side onto the back (posterior surface) of the ear.
- Position the ear. Gently hold the ear in the position you want, close to the head but not forced flat.
- Secure to the head. Peel the backing from the second side and press the corrector firmly against the skin behind the ear.
- Hold for 30 to 60 seconds. Light pressure from your fingertip helps the adhesive bond fully.
For removal, dab a small amount of baby oil around the edges of the corrector and let it soak in for a minute. Peel slowly and gently, holding the surrounding skin taut. A bit of temporary pinkness after removal is normal and typically fades within minutes.
What Results Can You Realistically Expect?
Non-surgical ear correction produces gradual, cosmetic improvement. You are not going to see an overnight transformation. Most parents begin noticing subtle changes after 2 to 3 weeks of consistent wear: the ear sits a little closer to the head, folds appear more defined, and the overall projection decreases.
Three factors determine the final result:
- Starting age: Earlier means faster, more predictable outcomes.
- Initial prominence: Mild to moderate cases tend to respond best.
- Consistency: Daily, round-the-clock wear is the single most important variable. Skipping days slows progress significantly.
A 10-year follow-up study on non-surgical ear molding confirmed that the cosmetic improvements achieved in infancy remained durable over time, with parents reporting sustained satisfaction years later. While no non-surgical method can guarantee the identical permanence of surgical reshaping, the evidence strongly supports lasting results when treatment is started early and applied consistently.
When to See a Doctor
Prominent ears are almost always a cosmetic concern, not a medical one. However, you should consult your pediatrician if:
- The ear shape appears significantly unusual (very small ears, missing structures, or closure of the ear canal).
- You have any concerns about your baby's hearing.
- Skin under or around a corrector shows persistent redness, bumps, or a rash that does not resolve with a 24-hour break.
- One ear looks dramatically different from the other in ways that go beyond simple prominence.
- You have used correctors consistently for 6 to 8 weeks with no visible change.
Your pediatrician can confirm the issue is cosmetic, rule out any underlying structural concerns, and give you a clear go-ahead for non-surgical correction. Many general pediatricians are already familiar with non-surgical ear molding as a technique, but if yours has not encountered it, you can explain that it is an at-home version of the same principles used in clinical neonatal ear molding programs at major pediatric hospitals. Most doctors are supportive of safe, non-invasive options that may help a child avoid surgery later.
Why DIY Taping Is Not the Same as Medical-Grade Correctors
Some parents try household tape or medical tape as a cost-saving measure. This is not recommended for several important reasons.
Standard tapes (surgical tape, micropore tape, athletic tape) are not engineered for long-term wear on infant skin. They lack the specific shape and structural support needed to hold the antihelical fold in the correct position. Without that targeted support, the ear may be held flat rather than guided into an anatomically natural curve, producing an unnatural result even if the tape stays on.
More critically, adhesives in standard tapes can cause irritation, rashes, or even blistering when worn continuously on delicate newborn skin. Babies have thinner, more permeable skin than adults, and prolonged contact with non-medical adhesives increases the risk of contact dermatitis.
Medical-grade correctors use dermatologist-tested, hypoallergenic silicone adhesive specifically formulated for continuous infant wear. The corrector shape is engineered to apply gentle pressure in the right places, encouraging the antihelical fold to develop naturally. The difference in safety, comfort, and effectiveness compared to household tape is substantial.
Where to Buy Baby Ear Correction Products
If you decide to try non-surgical correction, buy from a reputable source. Counterfeit ear correctors made with industrial-grade adhesives have been reported on third-party marketplaces, and they can cause serious skin reactions.
Your two safest options:
- The official brand website: Guaranteed authentic product, money-back guarantee, free shipping, and direct customer support.
- Amazon: Convenient and fast, but verify the seller is the official brand storefront on the product listing to avoid counterfeits.
Red flags for counterfeits include suspiciously low prices, unknown seller names, blurry product images, and poorly written listings.
Frequently Asked Questions
At what age can I start using ear correctors on my baby?
Most adhesive ear correctors designed for babies are suitable from around 3 months to 3 years old. The ideal window is as early as possible within that range, when the cartilage is still soft and pliable. If your baby is younger than 3 months, consult your pediatrician about clinical ear molding options available for newborns.
Will my baby's ears fix themselves without treatment?
Some minor folds from birth positioning may smooth out in the first few days. However, research shows that only about 30% of truly prominent ears self-correct. For the majority, the ear shape present in early infancy becomes permanent as the cartilage hardens.
Are ear correctors safe for my baby's skin?
Yes, when using a genuine medical-grade product. Look for correctors made from dermatologist-tested, hypoallergenic silicone with a skin-safe adhesive designed for continuous infant wear. Check the skin daily during changes. Mild pinkness after removal is normal. Persistent redness or irritation means you should give the skin a 24-hour break before reapplying.
How long does each corrector patch last before it needs replacing?
Each individual corrector typically stays on for 3 to 7 days, depending on your baby's skin type and activity level. Replace it when the edges begin to lift. Clean and dry the skin thoroughly before applying a fresh one.
Can my baby wear the correctors during baths and sleep?
Yes. Quality medical-grade correctors are waterproof and designed for 24/7 wear. They stay secure through baths, naps, overnight sleep, and playtime. Avoid scrubbing directly on the corrector during bath time, and pat the area dry afterward.
How long does the full treatment take?
For babies starting in the first few weeks of life, the typical treatment duration is 4 to 6 weeks. Starting later (3 to 6 months) generally requires 2 to 3 months of consistent wear. The key factor is daily, uninterrupted use.
Is non-surgical correction permanent?
Non-surgical molding produces cosmetic improvement, not a surgically guaranteed permanent change. That said, long-term follow-up studies show that results achieved during infancy, when the cartilage is soft, tend to be durable and lasting. The earlier you start and the more consistently you use the correctors, the better the long-term outcome.
How does this compare to otoplasty surgery?
Otoplasty is a surgical procedure requiring anesthesia, incisions, and recovery. It is typically performed after age 5 and costs $3,000 to $8,000 or more. Non-surgical correction is pain-free, non-invasive, and costs under $50. For many families, early non-surgical correction eliminates the need for surgery entirely. For a detailed comparison, see our EarFix vs. Surgery guide.
For Spanish-speaking families, we also have a dedicated guide: Corrector de Orejas para Bebes.